Parkinson’s Disease Overview
Parkinson disease (PD) is an adult-onset progressive neurodegenerative disorder, first described as “Shaking palsy” over 200 years ago by James Parkinson. While traditionally considered a motor system disorder based on the hallmark features of tremor, rigidity, and bradykinesia, PD is now recognized to be a complex disorder involving a wide range of nonmotor manifestations that contribute to disability.
The clinical features of PD arise partly from progressive degeneration of dopamine-producing neurons in the basal ganglia, including the substantia nigra in the midbrain, but degeneration of nondopaminergic neurons is implicated in many motor and nonmotor symptoms. Dopamine depletion and loss of other neurotransmitters account for the classic motor phenotype as well as a wide range of nonmotor and neuropsychiatric manifestations that affect function and quality of life.
5 Stages of Parkinson’s Disease Progression
In 1967, Hoehn & Yahr defined five stages of PD based on the level of clinical disability. Clinicians use it to describe how motor symptoms progress in PD. On this scale, stages 1 and 2 represent early-stage, stage 3 is considered transitional phase, and 4 and 5 advanced-stage PD.
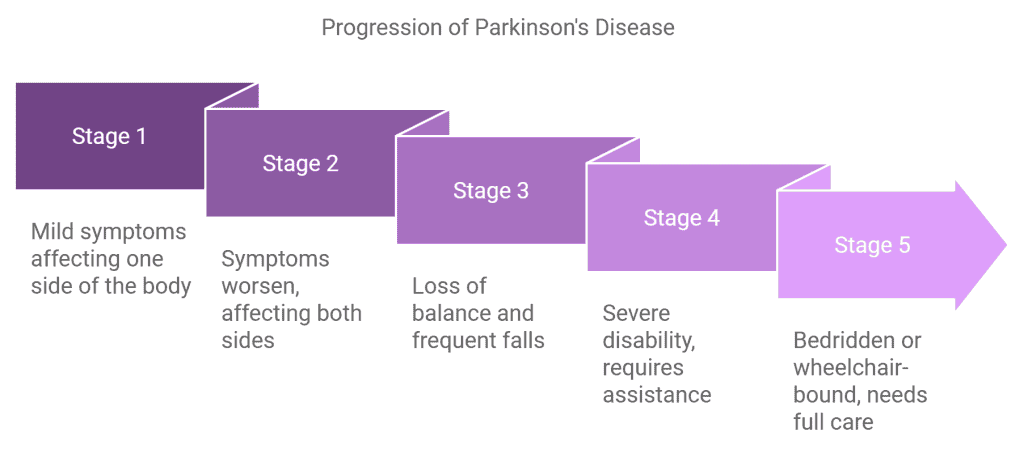
Parkinson’s Disease Psychosis (PDP), including hallucinations and delusions, typically presents in the transitional to advanced stages. While often associated with advanced disease—affecting up to 50% of patients in late stages—minor psychotic symptoms (such as presence hallucinations or illusions) can sometimes appear earlier and can predate motor symptoms in some patients.
Cognitive Impairment in Parkinson’s disease has a heterogeneous cognitive profile that is different from that of Alzheimer’s disease (AD). The general pattern is one of executive dysfunction and impaired visuospatial function, with less prominent memory deficits and relatively preserved language function. While PD can coexist with other common causes of dementia, such as Alzheimer’s disease and vascular dementia, cognitive impairment and dementia are increasingly recognized as a common feature of PD itself.
Clinical features of Parkinson’s disease dementia
| Cognitive features | Behavioral features |
|---|---|
|
|
A variety of neuropsychiatric and behavioral symptoms may occur in patients with PD; and while many such symptoms can occur in PD patients without dementia, they become increasingly common in patients with more severe cognitive impairment.
Put another way, Parkinson’s Disease Psychosis (hallucinations, delusions) may occur within a broader symptom set of cognitive impairment as disease progresses, or independently at earlier stages.
Clinical Manifestation and Causes of Parkinson’s Disease Psychosis
Parkinson’s Disease Psychosis (PDP) is characterized mainly by visual hallucinations and delusions, that are commonly paranoid in context.
Risk factors for PD psychosis include the prolonged use of anti-Parkinson drugs (i.e. dopamine agents), the presence of dementia, advanced age, impaired vision, depression, presence of sleep disorders, high comorbid disease burden, and longer disease duration. Psychosis can also be triggered by infection and acute episodes of delirium.
Visual hallucinations in PD are usually complex, involving well-formed images of people or animals. Duration and frequency are variable, but most hallucinations last for seconds to minutes. The prevalence and severity of hallucinations increase over time.
Many patients retain insight that their hallucinations are not real. However, patients with concomitant dementia or delirium may have decreased ability to ascertain reality, and these patients tend to be more resistant to treatment.
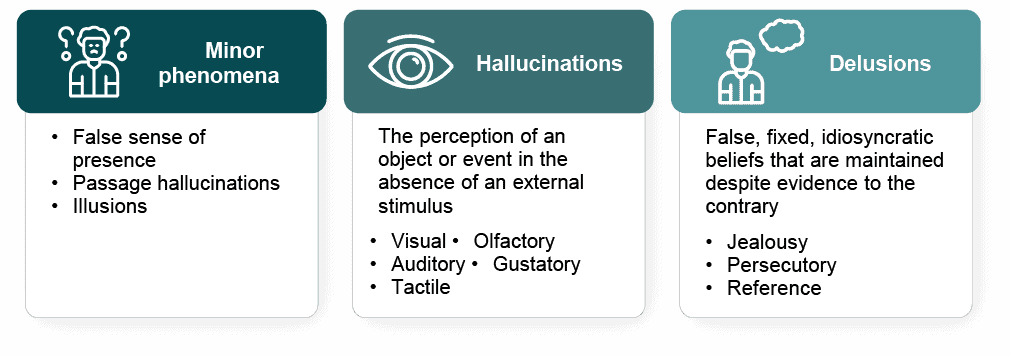
Delusions can also be a prominent feature of PD psychosis and are usually paranoid in nature. Common delusions include spousal infidelity, people stealing money, intruders living in the house, or caregivers planning harmful plots.
Psychosis, not motor dysfunction, is the single greatest risk factor for nursing home placement in patients with PD. Psychosis is also associated with increased caregiver burden and an increased risk of mortality.
Management of Parkinson’s Disease Psychosis (PDP) involves identifying and treating the underlying causes and contributory factors, including ruling out acute delirium.
Psychosis can be triggered by systemic conditions such as symptomatic or occult infection (e.g., pneumonia or urinary tract infection), so this possibility should be investigated and treated if present.
Anticholinergics can contribute to confusion and exacerbate PD psychosis. Psychoactive medications, including sedatives, anxiolytics, and antidepressants, may also contribute and should be reduced or stopped if possible.
Anti-Parkinson medication adjustments — Stopping all potentially offending anti-Parkinson drugs is generally not recommended, although dose reduction can frequently be accomplished with amelioration of hallucinations and limited loss of drug-related benefit.
Anti-Parkinson drugs may be reduced or stopped in an order that balances their efficacy in disease management and their likelihood of exacerbating or causing disabling hallucinations. For example, if a patient’s hallucinations began immediately after adding a COMT inhibitor (e.g. entacapone) to the combination of other drugs that had been previously well tolerated, then the COMT inhibitor should be stopped first.
If a temporal relationship is not clear, the suggested sequence of discontinuation begins with anticholinergic drugs, followed by amantadine, dopamine agonists, monoamine oxidase type B (MAO B) inhibitors, and COMT inhibitors. Levodopa should be considered for deprescribing last, since it is the most effective anti-Parkinson agent and least likely to cause psychosis. However, frequent and high-dose Levodopa can contribute to psychosis symptoms over time.
Prototypical dopamine (D2) receptor blocking agents (DRBAs) may cause parkinsonism on their own while decreasing efficacy of anti-Parkison agents and should be avoided in these patients. This includes first-and second-generation antipsychotics, certain antiemetic and prokinetic agents, most notably metoclopramide and prochlorperazine.
Other less commonly implicated classes of drugs include dopamine-depleting agents (e.g., tetrabenazine), certain mood stabilizers (e.g., valproate), antidepressants, and calcium channel blockers.
Medication Management – Refractory PD Psychosis
For patients with troublesome hallucinations or delusions despite anti-Parkinson medication adjustments, pharmacologic treatment directed at the psychotic symptoms are warranted. Pimavanserin (Nuplazid) is the only antipsychotic FDA approved to manage the hallucinations and delusions associated with PD psychosis.
Pimavanserin acts as an inverse agonist and antagonist with high affinity for 5-HT2A receptors; no affinity for 5-HT2B or dopaminergic (including D2), muscarinic, histaminergic, adrenergic receptors, or to calcium channels. This provides a more favorable safety profile compared to other dopamine blocking antipsychotics.
In clinical trials, pimavanserin significantly reduced the frequency and / or severity of hallucinations and delusions associated with PD psychosis without impacting motor function. See https://www.nuplazidhcp.com/ for additional information.
Among antipsychotics, clozapine and pimavanserin have the most evidence supporting efficacy; and while quetiapine is widely prescribed, data supporting its benefit in this patient cohort is lacking, with some studies indicating no benefit compared to placebo.
Elderly patients with dementia-related psychosis treated with any antipsychotic drug are at an increased risk of mortality and cardiovascular events. In patients with PD specifically, data also suggest that antipsychotic use is associated with an increased risk of mortality, morbidity and health care utilization. These risks must be balanced with the high morbidity and mortality of untreated psychosis.
Retrospective Claims Database Analyses: Healthcare Utilization Data
Acadia has recently funded a series of administrative claims database analyses to review healthcare utilization outcomes from Medicare claims to compare pimavanserin to other antipsychotics in management of PD psychosis, in terms of real-world outcomes. These studies are not randomized and observational in nature, the results describe associated risk and do not represent direct causality. A selection of conclusions from these analyses are provided below:
- Significantly lower all-cause and psychiatric hospital admission rates over 12 months compared to patients who initiated monotherapy with other atypical APs or quetiapine (on pimavanserin, PD psychosis).
- A significantly longer time to first LTC admission vs quetiapine patients; LTC admissions were found to be 10% lower among pimavanserin patients compared to other atypical APs and quetiapine (on pimavanserin, PD Psychosis).
- Significantly lower all-cause and psychiatric hospital admission rates for 6 months post-pimavanserin versus pre-pimavanserin initiation. (new diagnosis PDP)
- Significantly lower all-cause and psychiatric inpatient hospital admission rates over 6 months compared to residents who initiated other atypical APs or quetiapine (on pimavanserin, LTC residents with PDP).
- A lower relative risk of falls and fractures over 6 months for nursing home residents managed with pimavanserin for PD psychosis versus other typical antipsychotics or quetiapine.
These studies have limitations that are common to administrative claims database analyses. With any retrospective observational study design, causality cannot be inferred. To review these analyses and study design, see the resources linked below:
- Nuplazid (pimavanserin) Healthcare resource utilization studies[PN1.1]
- Fall and fracture findings in patients receiving Nuplazid (pimavanserin) for PDP[PN2.1]
References:
- UpToDate. Chou, Hurtig, Eichler. Clinical manifestations of Parkinson disease. Revised Nov, 2025. Subscription required to view.
- UpToDate. Chahine, Hurtig, Eichler. Management of nonmotor symptoms in Parkinson disease. Revised Feb, 2026. Subscription required to view.
- UpToDate. Rodnitzky, DeKosky, Wilterdink. Cognitive impairment and dementia in Parkinson disease. Revised Dec, 2024. Subscription required to view